The Four Guiding Principles For Democratizing IVF: Pre-ASRM 2022 Prep Notes From The Front Lines Of IVF Innovation
Ah, October in New York: crisp air, colorful trees against a royal blue sky. Shorts and t-shirts on Monday; sweaters and sweats on Tuesday. Juilliard students busking in Riverside Park; packed subways heading uptown for the Penn-Columbia football game.
Sorry, got carried away with that last one.
Since 1989, my October has meant prepping for the American Society of Reproductive Medicine (ASRM) meeting, which starts this Saturday. This year I have the privilege of teaching a course in preimplantation genetics for disease prevention with two superstars of genetic medicine, Andria Besser and Emily Mounts, and addressing the Society for Reproductive Endocrinology (SREI) on shifts in the IVF labor force.
Anaheim, here we come.
The pre-ASRM week is a good time to update our vision for the future of IVF, a project that I’ve worked on since a stint on the board of directors of RESOLVE, with a goal of ever improving, accessible and affordable IVF for anyone who needs it, anywhere in the world.
Last year we looked at back at our original seven assumptions for how to get there, and talked about private equity, machine learning and artificial intelligence, and what we learned about IVF delivery from COVID. This year I want to shift gears a bit discuss the underlying principles for a bigger, more effective, more inclusive IVF world.
The vision has a four part foundation:
1) Abandon the travel agent model of IVF patient care. Thirty years ago a long trip to Europe meant a travel agent booked your flights, your hotels, your tours and your museum entries, then handed you one bill with a large number at the bottom. Now we have the freedom (if we want it) to make our own choices and price shop. IVF patients will have the same freedom.
2) Ideally, there should be a gravitational pull for incumbents — RE’s, embryologists, IVF networks, payors — to adopt the innovation playbook technology and data-centric innovations that will make this vision a reality, an adoption that means more efficient delivery, lower cost of production and higher certainty, the “let’s engineer the hell out of IVF” strategy that we have been talking about for years. BUT — we can do it with them, or we can do it without them. We’ve learned from biology that a viable system needs collateral pathways around blockages and bottlenecks. I’ll be discussion one of those collateral pathways at the SREI meeting this weekend.
3) Our third principle is probably the most important: today’s highest pregnancy rates should be the floor for outcomes for the future. More accessible IVF cannot mean lower quality IVF. Cheaper cycles mean nothing unless translated into meaningful outcomes, and the only meaningful outcome to patients is a heathy baby. This is the underlying principle for my three key performance indicators for any aspect of this projects:
· dollars until baby
· time until baby
· life disruption to have a baby
— the same goals that IVF patients solve for when choosing whether to and where to undergo treatment.
4) Greater certainty, uniformly higher outcomes and improved data collection and analysis leads to actuarial quality data, which leads to better risk management which leads to paying (and getting paid) for outcomes, not cycles — you pay when the procedure works.
And, yes, I believe this is not only possible, but inevitable. The only question is how long it will take. I do think that population pressures will accelerate some version of this, as macro, policy concerns add another incentive to democratize IVF.
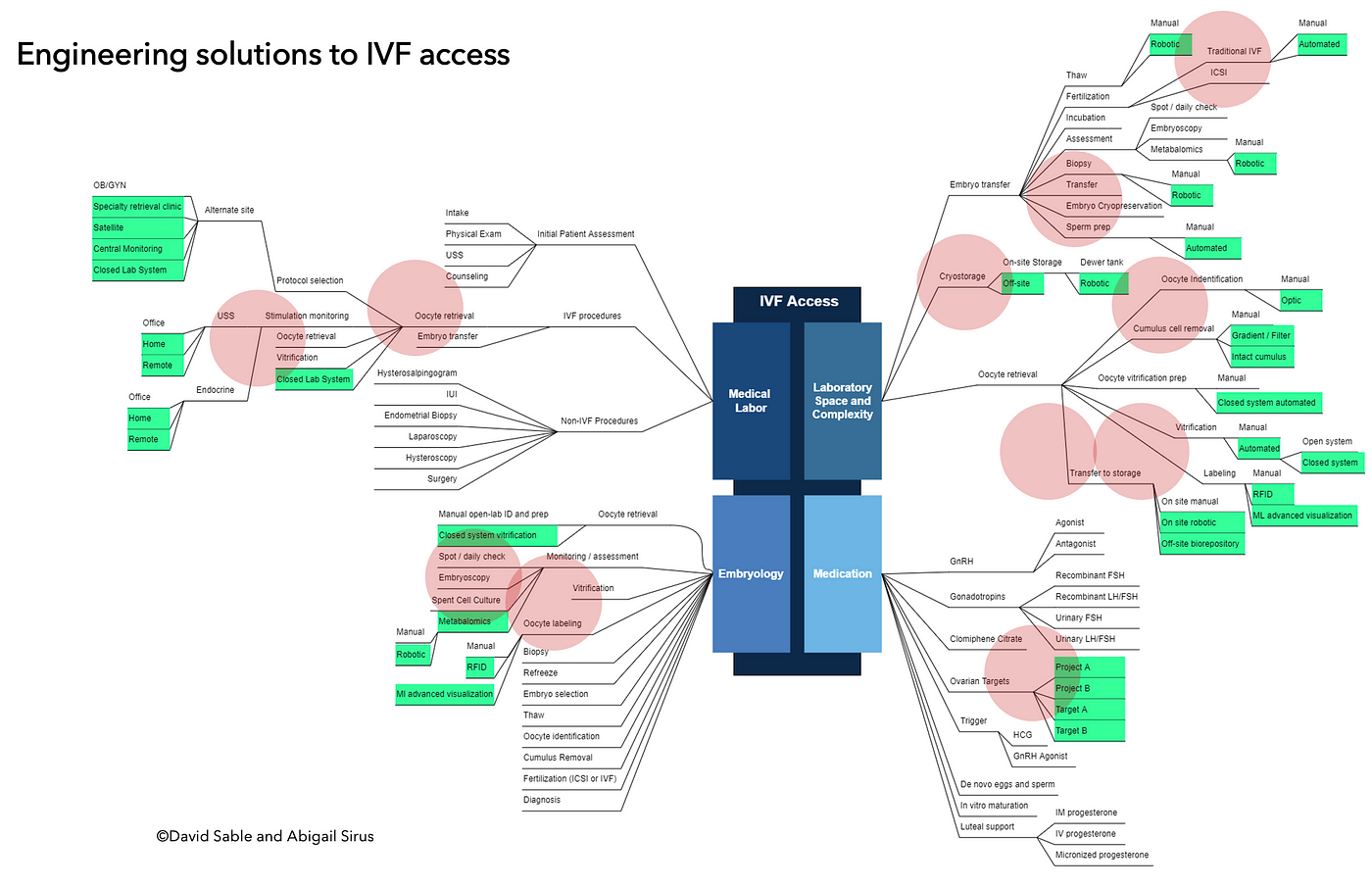
In the meantime, we’ve mapped out the specific blueprint to (what should we call it — IVF Extreme?) getting there. My colleague Abigail Sirus pictured it dramatically.
Not surprising, the inefficiencies in IVF can be grouped into four main areas:
1. REI’s spending too much time on the shop floor rather than in executive function
2. Underuse of embryology expertise in favor of embryology labor
3. Overuse of overbuilt and over-engineered laboratory space
4. Paying way too much for generic drugs
We found, as Abigail mapped so effectively, that grouping the steps in the IVF journey so that we could address several at once, a roadmap for using specific tools — AI, robotics, noninvasive diagnostics for home rather than office monitoring — emerged.
And this roadmap is our shopping list for allocating capital for IVF innovation for the future. If you’re in Anaheim next week (I’m there Saturday to Wednesday) stop me and say hello. We can talk about it.
